

Author: Arthi Adavikolanu
American High School, Fremont CA
February 28, 2021
Abstract
Substance abuse has continued to be a major public health concern for many years. Over the past couple decades, the rates for addiction have increased drastically, affecting many more women than before. A lot of these women are in their reproductive ages, pregnant, or soon-to-be-pregnant, and the constant abuse of these substances has a negative effect on the mother, her fetus, and, in the long term, her infant or child. Unfortunately, substance abuse during pregnancy is still very common. The effects of substance abuse are also not very well known to the public. These substances can easily pass through the placenta and reach the fetus, or even be transferred through the mother’s blood. Common effects on the fetus include preterm labor, intrauterine growth restriction, miscarriage, and internal defects. Many of these fetuses are also at high risk for developing neonatal abstinence syndrome, a withdrawal syndrome that occurs when the fetus is exposed to substances in utero. This review will target the effects of tobacco, alcohol, cocaine, and opioids on the mother, as well as immediate and long-term effects on her fetus.
Introduction
Substance use during pregnancy is a dangerous matter, resulting in harmful complications for both the mother and the fetus. The use of substances has increased drastically in the United States over the past 20 years, with tobacco leading as the most used substance during pregnancy, followed by alcohol, cannabis, and other prohibited drugs, including cocaine and opioids.[1] According to a survey in 2012, 5.9% of pregnant women used illegal drugs, 8.5% drank alcohol during pregnancy, and 15.9% used tobacco and cigarettes, causing over 380,000 offspring to be exposed to illicit substances, over 550,000 exposed to alcohol, and over one million exposed to tobacco in utero.[1] In 2014, 32,000 babies were born with neonatal abstinence syndrome[2,3], a post birth withdrawal syndrome that occurs due to a misuse of opioids during pregnancy. This was a five time increase from 2004[2], and a seven time increase from 2000.[3] A 2019 study showed that a baby is born with neonatal abstinence syndrome (NAS) about every fifteen minutes.[2]
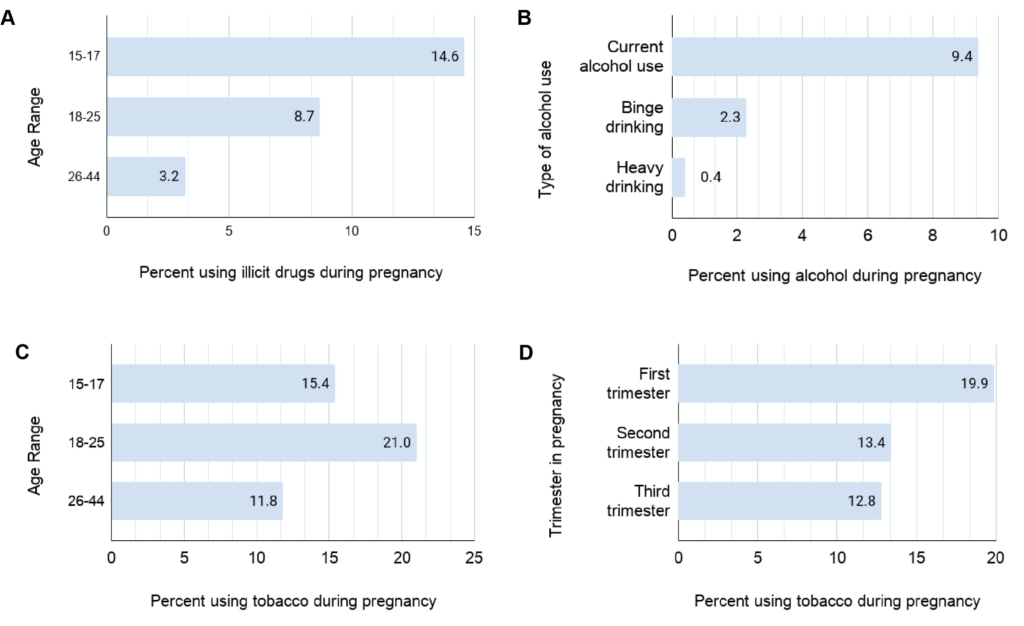
Women are a part of the 40% of those with a lifetime drug use disorder and 26% of those with both alcohol and drug abuse, causing women who are pregnant and soon-to-be pregnant to be placed at an increased risk for substance abuse.[1] Many women in their reproductive ages (18-29) were studied to have higher rates of abuse, furthermore affecting those who are pregnant or soon-to-be-pregnant.[1,4] Many girls (12-17) are also most likely to misuse illicit drugs.[5,6,7]
Many pregnant women also continued to use substances during pregnancy, as reported in a 2012-2013 study (Figure 1).[5]
Oxygen and nutrients easily pass through the placenta via the umbilical cord; all of these travel through blood circulation and feed the fetus to keep it healthy and alive. Similarly, any substance the mother intakes, including nicotine, carbon monoxide, tar, alcohol and illicit drugs, reaches the fetus through the umbilical cord, and it then enters the baby’s bloodstream[8,9] or crosses the blood-brain barriers, exposing fetuses in utero.[10]
Not only does substance abuse have unfavorable effects on the pregnancy and fetus, it also affects the economy poorly. In 2014, neonatal abstinence syndrome cost over $500 million in hospitalization costs.[2.3] The majority of these charges (82%) were paid by state Medicaid programs.[3] Alcohol addiction also costs a considerable amount of fines for medical care and affects people of all socioeconomic backgrounds.[11]
The risks and consequences of substance and polysubstance use, the consummation of more than one drug at once, have become a major public health concern over the past decade, due to the health effects and behavioral changes in the mother. Physical effects on the mother, such as miscarriage and preterm labor, also take place due to a dependency on substances.[12] The fetus undergoes possibilities of stillbirth, fetal growth restriction, prematurity, and neonatal abstinence syndrome[12]; however, the effects depend on the substances taken, the gestational period at which the fetus was susceptible to the substance, and the dosage taken by the mother.[13]
This review will focus on the effects of three major substances: tobacco, alcohol, and illicit drugs on the fetus, its mother, and its long-term development
2. Tobacco addiction
Tobacco and nicotine are leading avoidable causes of infant death, low birth weight, and premature births.[14] The mother’s smoking habits can cause major effects on the fetus, including facial defects and internal issues, and even on the infant such as mental disabilities and physical defects. It is estimated that 15 to 25% of women, who reported smoking before pregnancy, continue to smoke during pregnancy.[8] Smoking prevalence for females is also further affected by the maternal age and education level. Pregnant women over 35 years of age have reported to have been smoking less than those in their twenties and thirties (9% versus 20%, respectively). Furthermore, those with over 12 years of education were also shown to smoke less than those with less than ten years of education (6.5% compared to 22%, respectively).[14] Although cessation of smoking during the third semester has been linked to positive outcomes, very few women stop smoking, or stop for the pregnancy only to continue postpartum.[15]
Excessive smoking can cause poor nutrition in the mother, later affecting the blood flow to the placenta due to the nicotine exposure. The pregnancy could be affected since the tobacco smoke may cause intrauterine growth restriction or placental abruption, leading to preterm labor, increased risk of miscarriage, premature births and a fetus’s low birthweight.[16]
The effects of smoking on the fetus are very broad since cigarette smoke contains several different agents, such as carbon monoxide, metals, and nicotine, all known to be toxic to fetuses.[8,16] The principal adverse effects caused by tobacco exposure on the fetus’s health are reviewed in the following paragraphs.
2.1 Defects of the gastrointestinal system
Gastrointestinal defects include abdominal wall defects and a range of abnormalities of the pharynx, esophagus, intestine, colon, bile ducts, gallbladder, and liver.[14] However, out of thirty-five studies (11, 580 malformed cases, 9.7 million controls), most studies showed similarities in results.[14]
2.2 Facial defects
Facial defects include cleft lip or palate, as well as eye defects like optic nerve hypoplasia. Considering the studies from Hackshaw et al 2011 and Shi et al 2007, thirteen of thirty-eight studies (23, 441 malformed cases, 8.1 million controls) showed significant incidence of oral clefts in newborns exposed to tobacco, with six reporting evidence of dose-response relationship.[14,17] When eye defects were solely studied, five of nine studies (4, 541 malformed cases, 2.3 million controls) reported evidence of relation to maternal tobacco smoking during pregnancy.[14,18]
2.3 Musculoskeletal defects
Musculoskeletal defects include a variety of issues with limbs, bones, and muscles; underdevelopment of the hands and feet, as well as the radia, fibula, tibia, and ulna are all common risks with the musculoskeletal system. Eight studies (2915 malformed cases, 2.4 million controls) reported an increased risk for defects in the musculoskeletal system, with two studies showing significant prevalence of limb reduction disorders.[19] Tobacco use during pregnancy can also pose an increased risk of craniosynostosis, a birth defect in which the bones of the fetus’s skull conjoined too early, deforming the fetus’s head shape.[14]
2.4 Risk of cancer in early childhood
A clear correlation between smoking during pregnancy and risk of developing tumors during early childhood in the offspring has not been established yet. While an increase of brain tumors, tumors of the central nervous systems, and potential lymphomas have been associated to tobacco smoking during pregnancy[13], other forms of tumors, including leukemia, bone, soft tissue, renal, hepatic, and germ cell cancer cannot be associated to maternal smoking as a risk factor, due to the limited number of studies available.[20]
2.5 Psychological issues
Tobacco smoke and nicotine have also shown to be a cause for psychological problems such as attention-deficit/hyperactivity disorder (more commonly addressed as ADHD), depression, decreased adolescent happiness, disruptive behavioral disorders, and anxiety in offspring.[21,22,23,24] While maternal smoking can be correlated to these behavioral health issues, these factors are also deeply affected by maternal mental health and socioeconomic status. Furthermore, while there may be a drop in the adolescent’s happiness, there has been no direct correlation of maternal smoking with depression in the adolescent.[21] Eight of eleven studies reported an increased chance of infants developing ADHD from mothers who prenatally used nicotine.
While the influence of tobacco and nicotine so early in their development is yet to be fully determined, the physical and mental health of the infants are well monitored. Although there is extensive literature on the effects of tobacco and nicotine on the infant during development, there is a dearth of such resources on the long-term effects. Children exposed to tobacco and nicotine as infants have reported to be overweight, and show impulsivity, attention issues, and poor language and learning developments.[13] If not stopped, tobacco smoke and nicotine could cause severe maternal outcomes; therefore, recommending against smoking would severely help the course of the mother’s pregnancy, as well as the health of the infant. Many effective treatment options such as behavioral therapies, medications and interventions are available for pregnant women to help with tobacco cessation.
3. Alcohol addiction
Alcohol’s addictive structure and harmful nature make it a notable health problem. Alcohol can be an extremely dangerous substance, especially if taken in the first months of pregnancy. To create and maintain a healthy environment for the fetus to develop, a mother has to manage a healthy and safe diet. Alcohol leads to many complications in women: liver issues such as cirrhosis, heart problems such as damage to heart muscles, and an increase in cancer, most commonly, breast cancer.[25] The constant usage of alcohol could also lead to alcohol use disorder, which is a chronic relapse disorder in the brain that prevents someone from stopping or controlling their drinking.[26] Maternal alcohol consumption during the months before and during her pregnancy, even if moderate, can be linked with intrauterine growth restriction, caused by decreased cortisol activity [27] and an increased risk of preterm labor, miscarriage and stillbirth.[28] The most serious effects of maternal alcohol abuse on the fetus and on the infant are here summarized.
3.1 Fetal alcohol syndrome
With a mother’s dangerous intake of alcohol during pregnancy, a fetus could develop an irreversible syndrome termed as fetal alcohol syndrome (FAS), that causes problems in the central nervous system, physical and behavioral issues . Although the negative impact alcohol has on a fetus and infant are well-known, many women continue to drink throughout their pregnancy. In 2004, in the four million pregnancies, about 40% of those women drank alcohol during pregnancy, and another 3-5% of women drank heavily throughout their pregnancy.[27] People diagnosed with fetal alcohol syndrome disorder (FASD) have to receive lifelong assistance from a wide range of services including health, community, and remedial education, costing individuals around $1 million dollars.[11]
FAS is caused by the mother drinking large quantities of alcohol (100 mL a day or more) during the first few months of her pregnancy. It is characterized by microcephaly, growth restriction, mental retardation, behavioral disorders, cardiac defects, and facial defects.[1,9] If a mother drinks 30-60 mL of alcohol a day, minimal mental deficits, delayed growth, and behavioral disorders develop in the fetus.[9] FAS is the farthest on the FASD spectrum.[29]
A woman’s intake of alcohol in the months before and during her pregnancy are key factors that lead to FAS in the fetus.[1,9] Infants affected with FAS have a broad range of problems that arise during their childhood. Although there may be no current cure for FAS, doctors and scientists continue to study and monitor infants and children since the effects of FAS tend to last a lifetime. The effects of FAS are severe, but they can be avoided if mothers halt their intake of alcohol during the months of their pregnancy, since it can cause intrauterine growth restriction and prenatal death.
3.2 Effects on the brain and on the central nervous system
Alcohol exposure affects a fetus’s brain the most. The corpus callosum has been studied to be the most affected portion of the brain. The corpus callosum allows both sides of the brain to communicate, and the lack or partial absence of it can cause development problems, such as problems reading facial expression or difficulty with problem-solving and complex tasks.[27] Alcohol exposure also affects the central nervous system: dysfunctions in learning, emotion, cognition, motor performance, perception, and behavioral difficulties.[27] The subcortical region is also weakened, causing motor control, learning abilities, and behavioral inhibition.[27] The cavities, or ventricles, of the brain could also be affected, since there could be a buildup of spinal fluid in the brain, causing hydrocephalus.[13] Other brain defects include microcephaly, a condition in which the fetus’s head is smaller than average size.
3.3 Face and organ defects
Fetuses are also at risk for facial defects such as cleft lip, a low nasal bridge, and a flat midface.[13] Prenatal exposure also affects the heart; alcohol can cause cardiac deficits such as conotruncal anomalies. An example of a conotruncal anomaly is d-transposition of the great arteries (dTGA) in the fetus.[13,27] dTGA causes the aorta and pulmonary arteries to reverse roles, meaning the right ventricle is connected to the aorta and the pulmonary arteries are connected to the left ventricle. This pumps the blood in the wrong direction since the oxygenated blood flows to the lungs while the deoxygenated blood flows into the body. dTGA results in dangerous damage to the muscles of the heart.[27]
3.3 Behavioral issues
Infants exposed to alcohol in utero have shown to have high chances of developing irritability, which is a possible warning for a challenging temperament and behavioral issues during childhood.[30] Infants have also shown to have disturbed sleeping patterns and feeding difficulties.[30] A lower IQ has also been reported among infants exposed to alcohol perinatally.
3.4 Effects of alcohol abuse on the infant through breastfeeding
The use of alcohol in moderate amounts while breastfeeding should not impact the infant.[31,32] However, the mother’s intake of alcohol does change the odor of the breast milk, ultimately affecting how much milk the infant receives. It has been demonstrated that infants consume around 20% less milk after a period of three of four hours after a mother’s drinking.[33] This direct intake of alcohol can also impact the infant’s sleeping pattern. One case, reported by Anderson et al, 2018, showed violent fits and grand mal seizures as well as restlessness suffered from an infant breastfed by an alcoholic mother.[31] According to the Center for Disease Control and Prevention (CDC), women who may be or are pregnant should not be drinking at all, even in moderation.[34] If the mother is already at high levels of alcohol, there are many steps and interventions women could take to lessen the effects of their alcohol abuse or better understand handling a pregnancy with such issues. A woman could see if her child qualifies for an early intervention program that will help the child learn basic life functions such as walking and talking. There are other options such as medical care, medication for the child, education therapy, and parent training.[35] However, mothers should still be highly advised to stop drinking, resulting in a healthier and safer pregnancy for both the baby and the mother.
4. Illicit drug addiction
Drugs continue to harm many of its users and can easily cause death. According to the CDC, in 2018 over 67,000 deaths were reported due to drug overdose.[36] Many of these drugs are illegally manufactured, such as synthetic opioids, and others are illegally received, such as cocaine and heroin. The effects of these drugs on pregnant women are very dangerous, costing the life of both the mother and fetus. In this section, the effects of cocaine and opioids, two of the most dangerous drugs to a pregnancy, are described in detail.
4.1 Cocaine addiction
The use of cocaine has remained prevalent in the United States regardless of many attempts from the government and other non-profits to decrease substance abuse. Cocaine is approximately used by 2.8% of the population, and cocaine could be especially dangerous when used by a pregnant woman. Around 75% of women who use cocaine are of child-bearing age, and around 75,000 pregnancies are affected by a mother’s dangerous intake of cocaine throughout the pregnancy.[37]
Cocaine use can be extremely dangerous to a mother. Cocaine use also causes aggressive behavior, loss of muscle coordination, insomnia, and a large decrease in weight and nutrition.[9] In addition, it can cause neurological complications such as maternal migraines and seizures, dangerous cardiovascular issues, and sudden death.[9] Obstetric complications such as hypertension, difficult delivery, spontaneous miscarriage, and preterm labor, and separation of the placental lining from the uterus before delivery, postpartum hemorrhages, infections and fetal death are all prospective dangers to the mother.[9,38]
Cocaine remains to have a dangerous effect on fetuses. There is no definite pattern for the effects of cocaine, but chances of a fetus born with a cleft lip increase, especially when the mother uses during the third trimester of pregnancy.[13] Fetuses prenatally exposed to cocaine in the utero tend to have a higher chance of cardiovascular issues.[9,13] Fetuses have higher odds of developing arrhythmias, decreased cardiac output, heart disease, and transient myocardial ischemia.[39] Cocaine also affects the kidneys since cocaine reduces the blood flow to the fetus. The kidney can swell due to this lack of blood supply, and the urine backs up, causing hydronephrosis.[40] Cocaine can also affect the fetus’s development of the brain, by preventing the development of the neurological nerves and causing the death of certain regions of the brain.[40] Also, according to Stanford, cocaine affects the fetus itself more than it causes a withdrawal, an effect of neonatal abstinence syndrome (NAS), at birth.[41]
Infants and children exposed to cocaine neonatally have many complications that extend after birth. Children tend to exhibit signs of irritability and hypertonia, the inability of a muscle to stretch. Children also tend to have a lower attention span[13,40] and the inability to retain visual memories. Children lacked visual-motor skills and had subtle language delay[13], caused by the damages of distinct areas of the brain. Prenatal cocaine use also affects a child’s IQ, and some children have a reduced intellectual capability.[13,40]
4.2 Opioid addiction
Opioids are a class of drugs that include heroin, synthetic opioids such as fentanyl, and legal painkillers such as morphine and Vicodin. For example, fentanyl is a legally distributed painkiller produced by pharmaceutical companies but also an illicitly manufactured opioid, yet it has caused an increase in overdose deaths due to opioids by 10%.[42] Opioids have been a majorly used drug group in the United States. In 2018, 47,000 overdoses involved opioids, and 32% of these deaths were a result of prescription opioids.[42,43] One in three women in the reproductive age have been prescribed opioids between 2008 and 2012[44], and in 2019, one in five women reported to have used opioids during pregnancy for other reasons other than to relieve pain, such as to aid their addiction.[45,46]
Opioids are most usually prescribed to a woman to relieve pain or received illegally. However, the effects of opioids on mothers are just as dangerous. Due to a misuse of opioids, a mother could develop opioid use disorder (OUD), which causes extreme usage of opioids. According to the American College of Obstetricians and Gynecologists, it is a chronic disorder and linked to the inability to control a craving for opioids.[47] This could lead to severe impairment of the brain as well as distress.[45] Furthermore, opioid use disorder is also a growing cause for maternal death during a pregnancy, causing over 1,200 deaths related to OUD.[48] A pregnant woman using opioids could suffer from respiratory failure[9], or experience potential obstetric complications such as spontaneous abortion, preeclampsia, placental abruption, and fetal death.[10,45] Furthermore, women who suffer from opioid abuse also suffer from depression, trauma, and anxiety.[47] Due to opioid abuse, over 30% of pregnant women were reported to have moderate to severe depression, and over 40% showed symptoms of postpartum depression six weeks after delivery.[47,49]
The usage of opioids has also been linked to congenital abnormalities in the fetus. Firstly, since opioids flow easily through the placenta to the fetus, the fetus is highly likely to become addicted to the substance the mother is using in utero. This can lead to NAS, causing tremors, seizures, sleep problems, and more problems postnatally. The fetus is also at high risk for death due to the mother’s withdrawal episodes. Opioid addiction can also cause intrauterine growth restriction as well as lower birthweight and preterm birth.[45,50]
Infants affected by uterine exposure to opioids are still affected by NAS, meaning that they will continue to have seizures, respiratory defects, and feeding difficulties.[51] Studies have also shown that children affected by NAS are more likely to develop a speech impairment as well as cognitive and neurodevelopmental issues.[52] Memory problems as well as hyperactivity have been examined in older children.[13] However, there is a lack of well documented data regarding opioid effects on infants and children.
Drug addiction is still a major issue for many people. It is severely dangerous for pregnant women, since the constant use of drugs is a health concern for the mother and the baby. There are many treatment options available to women who are addicted, but the treatment is extremely tough, and relapse is very common. Some treatment options include behavioral counseling, medication, and some medical devices to help with withdrawal. Although difficult, a woman should try to refrain from drug use or receive help regarding her addiction for the safety of her and her baby.
Conclusion
The effects of substances have caused congenital anomalies and many defects very commonly. In order to safeguard the health of the mother and her child, a mother using the substances described in this review should often get ultrasounds as well as meet with her doctor to monitor the progress of her pregnancy. If the mother continues to abuse substances during her pregnancy, her fetus and child will be severely impacted, and many long-term effects can affect the child’s physical and mental health. The child may also develop many psychological and mental disabilities that affect their intellectual ability to perform. Prevention of these substances during pregnancy will help the chances of her and her baby having a successful birth as well as a healthy future. Furthermore, there are many treatment options to consider during pregnancy as well as post-pregnancy. The mother could receive assistance to cease her addiction while the child could receive help on handling the disabilities that may arise with the mother’s addiction. In conclusion, substance abuse should be strongly advised against during pregnancy.
References
- Forray A. (2016). Substance use during pregnancy. F1000Research, 5, F1000 Faculty Rev-887. https://doi.org/10.12688/f1000research.7645.1
- NIDA. 2020, May 29. What are the effects of maternal cocaine use?. Retrieved from https://www.drugabuse.gov/publications/research-reports/cocaine/what-are-effects-maternal-cocaine-use on 2021, February 27
- Jansson, L. M., & Patrick, S. W. (2019). Neonatal Abstinence Syndrome. Pediatric clinics of North America, 66(2), 353–367. https://doi.org/10.1016/j.pcl.2018.12.006
- Compton, W. M., Thomas, Y. F., Stinson, F. S., & Grant, B. F. (2007). Prevalence, Correlates, Disability, and Comorbidity of DSM-IV Drug Abuse and Dependence in the United States. Archives of General Psychiatry, 64(5), 566. https://doi.org/10.1001/archpsyc.64.5.566
- Results from the 2013 NSDUH: Summary of National Findings, SAMHSA, CBHSQ. (2014). Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm#4.3
- Bezrutczyk, D., & Hampton, D. (2020, November 20). The Differences in Addiction Between Men and Women. Addiction Center. https://www.addictioncenter.com/addiction/differences-men-women/
- Becker, J. B., McClellan, M. L., & Reed, B. G. (2017). Sex differences, gender and addiction. Journal of neuroscience research, 95(1-2), 136–147. https://doi.org/10.1002/jnr.23963
- Wickström R. (2007). Effects of nicotine during pregnancy: human and experimental evidence. Current neuropharmacology, 5(3), 213–222. https://doi.org/10.2174/157015907781695955
- Hetea, A., Cosconel, C., Stanescu, A., & Simionescu, A. A. (2019). Alcohol and Psychoactive Drugs in Pregnancy. Maedica, 14(4), 397–401. https://doi.org/10.26574/maedica.2019.14.4.397
- Lind, J. N., Interrante, J. D., Ailes, E. C., Gilboa, S. M., Khan, S., Frey, M. T., Dawson, A. L., Honein, M. A., Dowling, N. F., Razzaghi, H., Creanga, A. A., & Broussard, C. S. (2017). Maternal Use of Opioids During Pregnancy and Congenital Malformations: A Systematic Review. Pediatrics, 139(6), e20164131. https://doi.org/10.1542/peds.2016-4131
- Popova, S., Lange, S., Shield, K., Mihic, A., Chudley, A. E., Mukherjee, R., Bekmuradov, D., & Rehm, J. (2016). Comorbidity of fetal alcohol spectrum disorder: a systematic review and meta-analysis. Lancet (London, England), 387(10022), 978–987. https://doi.org/10.1016/S0140-6736(15)01345-8
- Pinto, S. M., Dodd, S., Walkinshaw, S. A., Siney, C., Kakkar, P., & Mousa, H. A. (2010). Substance abuse during pregnancy: effect on pregnancy outcomes. European Journal of Obstetrics & Gynecology and Reproductive Biology, 150(2), 137–141. https://doi.org/10.1016/j.ejogrb.2010.02.026
- Soto, E., Bahado-Singh, R., Christensen, C., Chauhan, S., Sibai, B., & Viteri, O. (2014). Fetal Anomalies and Long-Term Effects Associated with Substance Abuse in Pregnancy: A Literature Review. American Journal of Perinatology, 32(05), 405–416. https://doi.org/10.1055/s-0034-1393932
- Hackshaw, A., Rodeck, C., & Boniface, S. (2011). Maternal smoking in pregnancy and birth defects: a systematic review based on 173 687 malformed cases and 11.7 million controls. Human reproduction update, 17(5), 589–604. https://doi.org/10.1093/humupd/dmr022
- Crume T. (2019). Tobacco Use During Pregnancy. Clinical obstetrics and gynecology, 62(1), 128–141. https://doi.org/10.1097/GRF.0000000000000413
- Smoking During Pregnancy. (2019, May 29). Centers for Disease Control and Prevention. https://www.cdc.gov/tobacco/basic_information/health_effects/pregnancy/index.htm
- Shi, M., Christensen, K., Weinberg, C. R., Romitti, P., Bathum, L., Lozada, A., Morris, R. W., Lovett, M., & Murray, J. C. (2007). Orofacial cleft risk is increased with maternal smoking and specific detoxification-gene variants. American journal of human genetics, 80(1), 76–90. https://doi.org/10.1086/510518
- Tornqvist, K., Ericsson, A., & Källén, B. (2002). Optic nerve hypoplasia: Risk factors and epidemiology. Acta Ophthalmologica Scandinavica, 80(3), 300–304. https://doi.org/10.1034/j.1600-0420.2002.800313.x
- Källén K. (2000). Multiple malformations and maternal smoking. Paediatric and perinatal epidemiology, 14(3), 227–233. https://doi.org/10.1046/j.1365-3016.2000.00269.x
- Rumrich, I. K., Viluksela, M., Vähäkangas, K., Gissler, M., Surcel, H. M., & Hänninen, O. (2016). Maternal Smoking and the Risk of Cancer in Early Life – A Meta-Analysis. PloS one, 11(11), e0165040. https://doi.org/10.1371/journal.pone.0165040
- Tiesler, C. M. T., & Heinrich, J. (2014). Prenatal nicotine exposure and child behavioural problems. European Child & Adolescent Psychiatry, 23(10), 913–929. https://doi.org/10.1007/s00787-014-0615-y
- Brion, M. J., Victora, C., Matijasevich, A., Horta, B., Anselmi, L., Steer, C., Menezes, A. M., Lawlor, D. A., & Davey Smith, G. (2010). Maternal smoking and child psychological problems: disentangling causal and noncausal effects. Pediatrics, 126(1), e57–e65. https://doi.org/10.1542/peds.2009-2754
- Herrmann, M., King, K., & Weitzman, M. (2008). Prenatal tobacco smoke and postnatal secondhand smoke exposure and child neurodevelopment. Current Opinion in Pediatrics, 20(2), 184–190. https://doi.org/10.1097/mop.0b013e3282f56165
- Huizink, A. C., & Mulder, E. J. (2006). Maternal smoking, drinking or cannabis use during pregnancy and neurobehavioral and cognitive functioning in human offspring. Neuroscience and biobehavioral reviews, 30(1), 24–41. https://doi.org/10.1016/j.neubiorev.2005.04.005
- Excessive Alcohol Use and Risks to Women’s Health | CDC. (2020, October 23). Center for Disease Control and Prevention. https://www.cdc.gov/alcohol/fact-sheets/womens-health.htm#
- Women and Alcohol | National Institute on Alcohol Abuse and Alcoholism (NIAAA). (n.d.). National Institute on Alcohol Abuse and Alcoholism. Retrieved January 10, 2021, from https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/women-and-alcohol
- Caputo, C., Wood, E., & Jabbour, L. (2016). Impact of fetal alcohol exposure on body systems: A systematic review. Birth Defects Research Part C: Embryo Today: Reviews, 108(2), 174–180. https://doi.org/10.1002/bdrc.21129
- Dejong, K., Olyaei, A., & Lo, J. O. (2019). Alcohol Use in Pregnancy. Clinical obstetrics and gynecology, 62(1), 142–155. https://doi.org/10.1097/GRF.0000000000000414
- Scott-Goodwin, A. C., Puerto, M., & Moreno, I. (2016). Toxic effects of prenatal exposure to alcohol, tobacco and other drugs. Reproductive Toxicology, 61, 120–130. https://doi.org/10.1016/j.reprotox.2016.03.043
- Kelly, S. J., Day, N., & Streissguth, A. P. (2000). Effects of prenatal alcohol exposure on social behavior in humans and other species. Neurotoxicology and teratology, 22(2), 143–149. https://doi.org/10.1016/s0892-0362(99)00073-2
- Anderson P. O. (2018). Alcohol Use During Breastfeeding. Breastfeeding medicine : the official journal of the Academy of Breastfeeding Medicine, 13(5), 315–317. https://doi.org/10.1089/bfm.2018.0053
- Haastrup, M. B., Pottegård, A., & Damkier, P. (2014). Alcohol and breastfeeding. Basic & clinical pharmacology & toxicology, 114(2), 168–173. https://doi.org/10.1111/bcpt.12149
- Mannella J. (2001). Alcohol’s effect on lactation. Alcohol research & health : the journal of the National Institute on Alcohol Abuse and Alcoholism, 25(3), 230–234.
- Facts about moderate drinking | CDC. (n.d.). Centers for Disease Control and Prevention. Retrieved January 10, 2021, from https://www.cdc.gov/alcohol/fact-sheets/moderate-drinking.htm
- FASDs: Treatments. (2021, January 27). Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/fasd/treatments.html
- Drug Overdose Deaths | Drug Overdose | CDC Injury Center. (n.d.). Centers for Disease Control and Prevention. Retrieved January 10, 2021, from https://www.cdc.gov/drugoverdose/data/statedeaths.html
- Substance Use While Pregnant and Breastfeeding. (2020, June 6). National Institute on Drug Abuse. https://www.drugabuse.gov/publications/research-reports/substance-use-in-women/substance-use-while-pregnant-breastfeeding
- What are the effects of maternal cocaine use? (2020, May 29). National Institute on Drug Abuse. https://www.drugabuse.gov/publications/research-reports/cocaine/what-are-effects-maternal-cocaine-use
- Meyer, K. D., & Zhang, L. (2009). Short- and long-term adverse effects of cocaine abuse during pregnancy on the heart development. Therapeutic advances in cardiovascular disease, 3(1), 7–16. https://doi.org/10.1177/1753944708099877
- Tantibanchachai, C. M. Z., & Zhang, M. (2013, October 17). Cocaine as a Teratogen | The Embryo Project Encyclopedia. The Embryo Project Encyclopedia. https://embryo.asu.edu/pages/cocaine-teratogen
- Stanford Children’s Health. (n.d.). Stanford Children’s Health. Retrieved January 13, 2021, from https://www.stanfordchildrens.org/en/topic/default?id=neonatal-abstinence-syndrome-90-P02387
- Wilson, N., Kariisa, M., Seth, P., Smith, H., & Davis, N. L. (2020). Drug and Opioid-Involved Overdose Deaths — United States, 2017–2018. MMWR. Morbidity and Mortality Weekly Report, 69(11), 290–297. https://doi.org/10.15585/mmwr.mm6911a4
- Data and Statistics About Opioid Use During Pregnancy | CDC. (2020, August 13). Centers for Disease Control and Prevention. https://www.cdc.gov/pregnancy/opioids/data.html
- Ailes, E. C., Dawson, A. L., Lind, J. N., Gilboa, S. M., Frey, M. T., Broussard, C. S., Honein, M. A., & Centers for Disease Control and Prevention (CDC) (2015). Opioid prescription claims among women of reproductive age–United States, 2008-2012. MMWR. Morbidity and mortality weekly report, 64(2), 37–41.
- Basics About Opioid Use During Pregnancy | CDC. (2020, November 25). Centers for Disease Control and Prevention. https://www.cdc.gov/pregnancy/opioids/basics.html
- Ko, J. Y., D’Angelo, D. V., Haight, S. C., Morrow, B., Cox, S., Salvesen von Essen, B., Strahan, A. E., Harrison, L., Tevendale, H. D., Warner, L., Kroelinger, C. D., & Barfield, W. D. (2020). Vital Signs: Prescription Opioid Pain Reliever Use During Pregnancy — 34 U.S. Jurisdictions, 2019. MMWR. Morbidity and Mortality Weekly Report, 69(28), 897–903. https://doi.org/10.15585/mmwr.mm6928a1
- Opioid Use and Opioid Use Disorder in Pregnancy. (2017, August). ACOG. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/08/opioid-use-and-opioid-use-disorder-in-pregnancy
- Mitra, A., Brandt, J., Rosen, T., Ananth, C., & Schuster, M. (2020). Opioid Use Disorder. Obstetrics & Gynecology, 135, 56S. https://doi.org/10.1097/01.aog.0000663364.06637.15
- Holbrook, A., & Kaltenbach, K. (2012). Co-occurring psychiatric symptoms in opioid-dependent women: the prevalence of antenatal and postnatal depression. The American journal of drug and alcohol abuse, 38(6), 575–579. https://doi.org/10.3109/00952990.2012.696168
- Reddy, U. M., Davis, J. M., Ren, Z., Greene, M. F., & Opioid Use in Pregnancy, Neonatal Abstinence Syndrome, and Childhood Outcomes Workshop Invited Speakers (2017). Opioid Use in Pregnancy, Neonatal Abstinence Syndrome, and Childhood Outcomes: Executive Summary of a Joint Workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, American College of Obstetricians and Gynecologists, American Academy of Pediatrics, Society for Maternal-Fetal Medicine, Centers for Disease Control and Prevention, and the March of Dimes Foundation. Obstetrics and gynecology, 130(1), 10–28. https://doi.org/10.1097/AOG.0000000000002054
- Patrick, S. W., Davis, M. M., Lehmann, C. U., & Cooper, W. O. (2015). Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012. Journal of perinatology : official journal of the California Perinatal Association, 35(8), 650–655. https://doi.org/10.1038/jp.2015.36
- Fill, M. A., Miller, A. M., Wilkinson, R. H., Warren, M. D., Dunn, J. R., Schaffner, W., & Jones, T. F. (2018). Educational Disabilities Among Children Born With Neonatal Abstinence Syndrome. Pediatrics, 142(3), e20180562. https://doi.org/10.1542/peds.2018-0562
About the author
Arthi Adavikolanu
Arthi is a student at the American High School, in Fremont, California.